One of the areas of interests of REHAssist are developments of accessible and cost effective rehabilitation techniques, that may easily be combined to conventional therapies. Powered robotic devices are not used, this makes the implementation in financial-constrained contexts easier.
The modalities considered by our group are as follows:
- Functional electrical stimulation
- Haptic feedback and sensory substitution
- Error augmentation
- BMI using EEG
Projects
- Balance Rehabilitation using error augmentation
- Non Invasive sFES for gait rehabilitation in inviduals with spinal cord injury, without and with BMI
Modalities and devices
Functional electrical stimulation
 |
Surface Functional Electrical Stimulation (sFES) in lower limb rehabilitation to in paraplegic patients has been widely studied. Numerous studies have shown its positive effects for SCI patients, such as maintaining or increasing muscle masses, promoting neuroplasticity, improving blood circulation, and reducing muscle spasticity. |
|
The StimWave is a custom electrostimulator, developed by our laboratory. It generates up to 100 mA simple periodic current pulses. The signal frequency is adjustable from 10 to 85 Hz and the pulse width from 100 to 300 microseconds. |
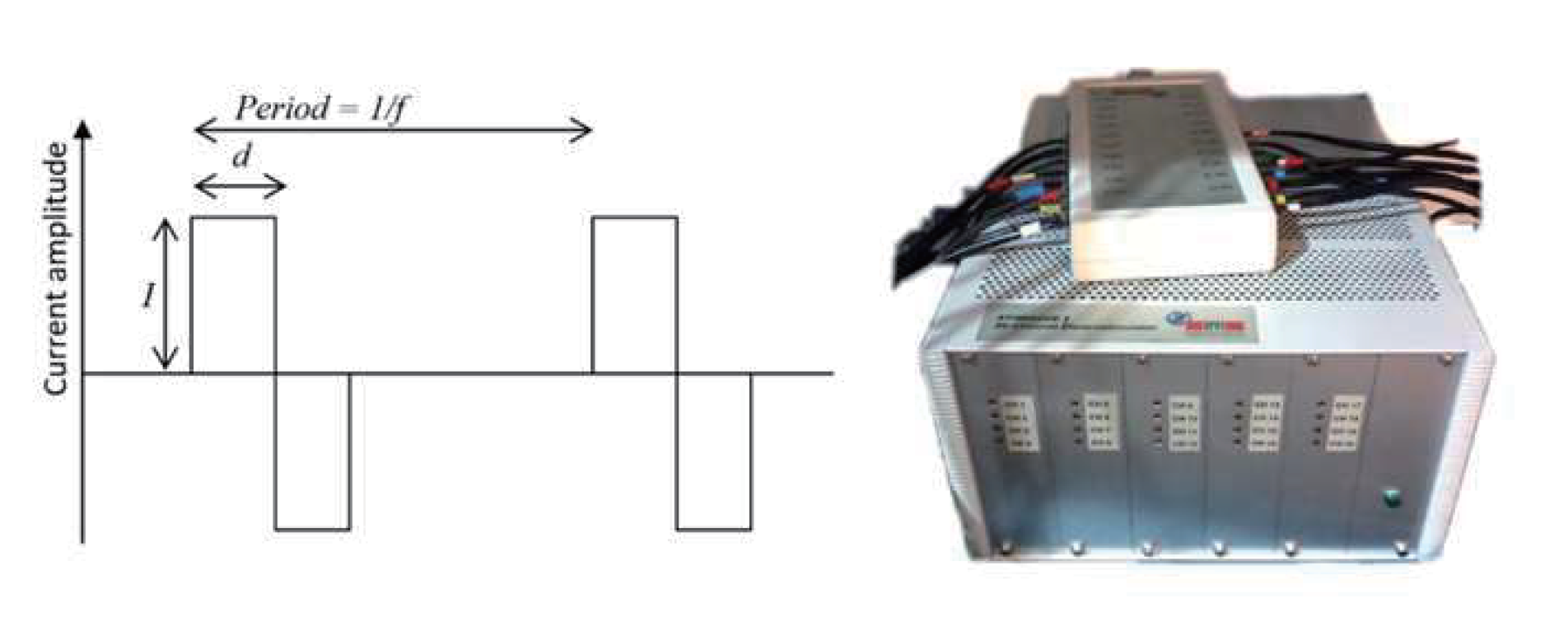 |
| XStim- A new generation of functional electrostimulation has been developed. XStim provides different electrostimulation modes: 1) simplet electrostimulation, generating only one programmable periodic pulse 2) doublet, generating 2 simultaneous periodic programmable pulses and 3) triplet, generating 3 simultaneous periodic programmable pulses. XStim has mainly been developed fr wearable application. | 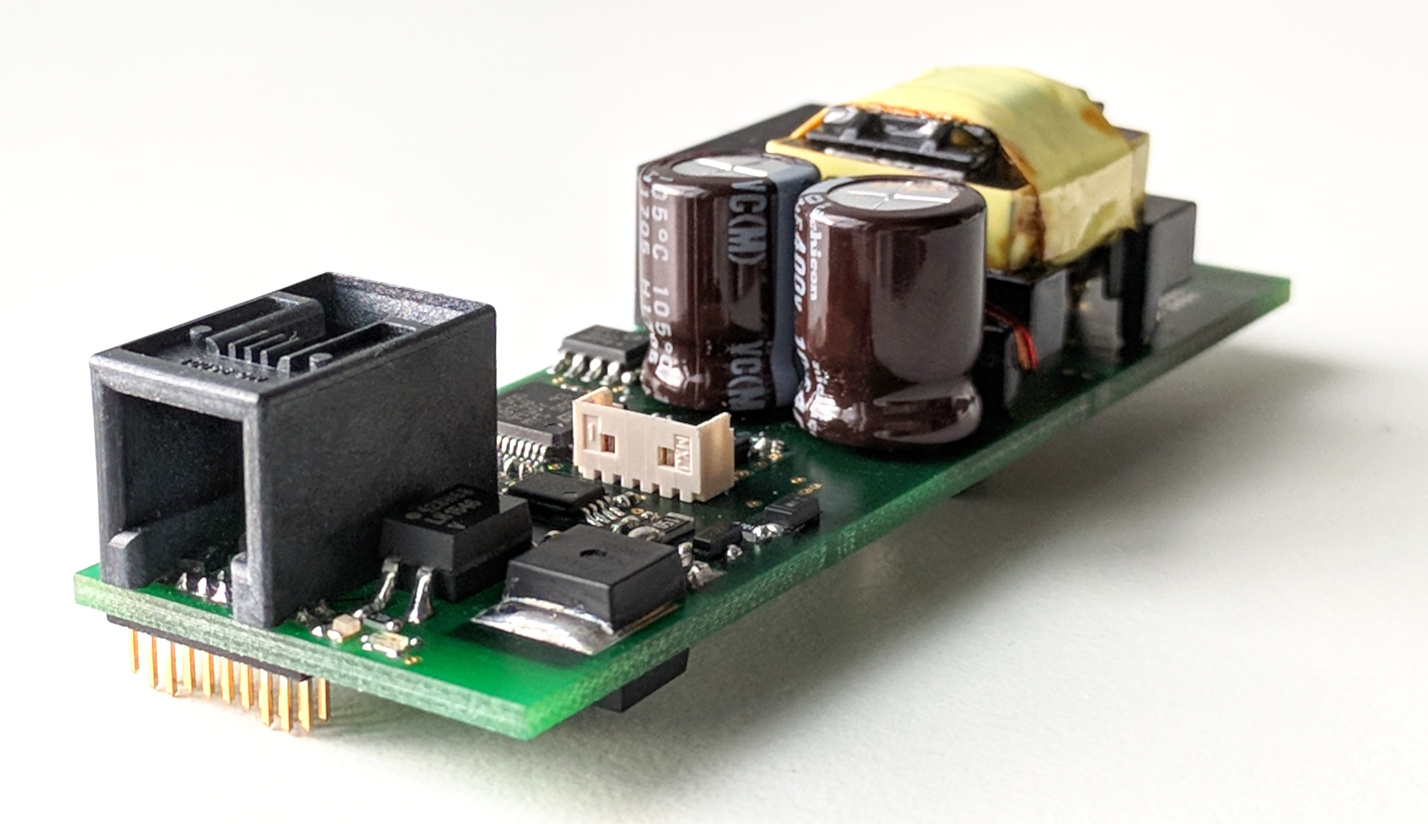
1-channel electrostimulator |
BMI using EEG for lower limb intention decoding
|
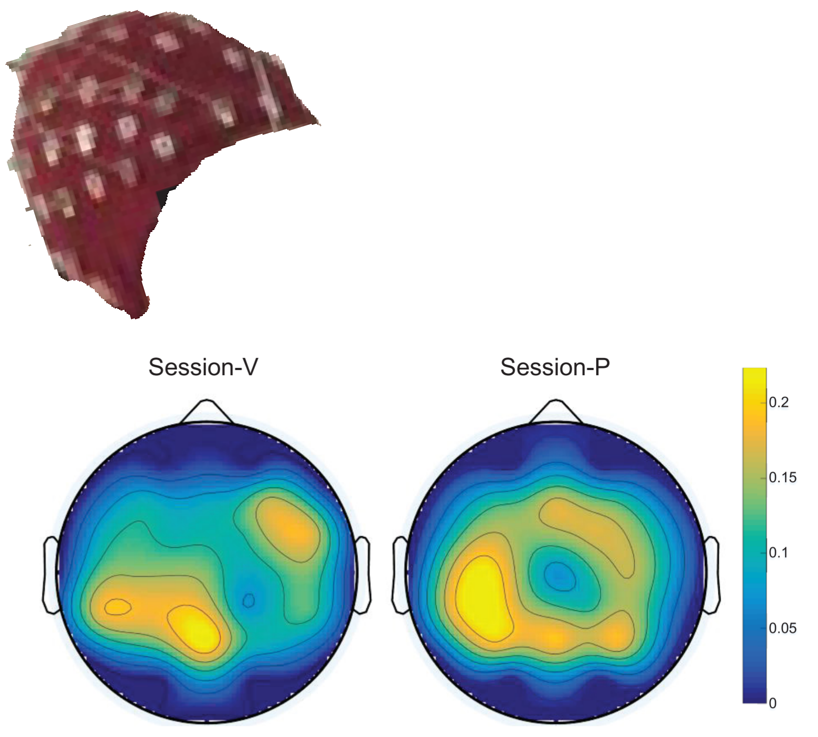
Electroencephalography (EEG)-based brain-machine interfaces (BMIs) have been developed to decode cerebral activities to detect motor activity and human intentions. The motor imagery (MI) is the most commonly implemented neural correlates for neurorehabilitation. Typically exploited motor intentions are imaging the kinaesthetic movements of 1)the left, respectively the right hand or both 2) foot/feet movements. In gait rehabilitation-oriented BMI, lower-limb MI is an intuitive yet challenging method, due to the relatively small brain region representing leg movements. In this topic, our group collaborates with Jose Milan lab and the neuro-rehabilitation center AASDAP. |
 |
Related publications:
Liu, Dong, et al. “Brain-actuated gait trainer with visual and proprioceptive feedback.” Journal of neural engineering 14.5 (2017).
Liu, Dong, et al. “EEG-based lower-limb movement onset decoding: Continuous classification and asynchronous detection.” IEEE Trans. on Neur. Syst. and Rehab Eng.(2018).
Vibrotactile haptic feedback
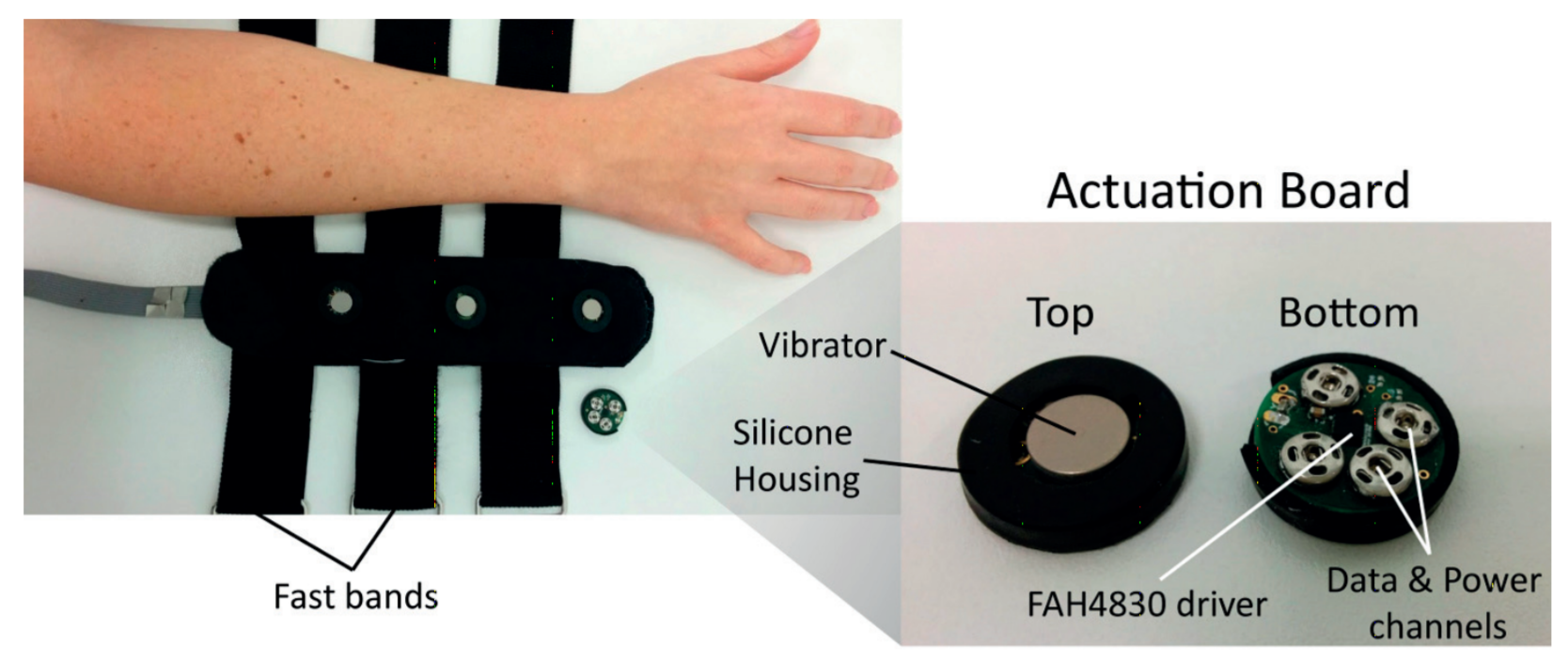 |
Sensory substitution concerns the the stimulation of one sense in an attempt to imitate the missing sensations of another sense [Paul Bach-y Rita, 1967]. In this case, the haptic channel is used as a substitute input channel to provide the information missing from damaged senses, such as vision, audition or spatial orientation. For individuals with SCI, who lost their sensations in lower limbs, we use sleeves equipped with vibrotactile actuators to feedback vibrations in specific sequences, when walking, in swing phases and in stance. The tactile display may be integrated in different garments. In suitable sleeves, taking advantage of an elastic compression, this may offer a offering a repetitive placement of the actuators. Patches featuring velcro fast bands for a fast placement and a good control over the contact force. |
Related publications:
Somon Gallo, “Wearable multimodal tactile interfaces for augmenting haptic perception.”, PhD Thesis dissertation, EPFL (2016).