Microsurgery is a particularly high-risk, high-stakes specialty with little margin for error and training of microsurgeons to ensure the highest quality of care and to minimize patient safety concerns may be of vital importance. Consequently, demonstration of measurable performance is important in order to evaluate skill acquisition and apply targeted feedback to improve training.

An ideal microsurgery assessment tool should be able to deconstruct all the subskills of microsurgery, to assess them objectively and reliably, and to show a good correlation between this assessment and outcome.
In this project, we will focus on:
- Visuo-spatial ability, which relates to the capacity to understand and remember the spatial relations among objects or space. This ability is required in vessel-wall dissection, suture-placement, and knot-tightening. The placement and spacing of sutures require visuo-spatial awareness to avoid catching the back-wall and suture entanglement. Lastly, knot-tying and knot-tightening under the microscope is also done under vision rather than by feel.
- Dexterity, which is the basic prerequisite for a microsurgical procedure and it relates to hand steadiness, flow of movements, finesse of surgery, instrument handling and tissue handling. Steadiness, i.e. absence of tremor, is a prerequisite to handle micro-instruments comfortably. Dexterous tissue handling is of importance to minimize tissue damage, which translates to a reduced risk of vessel thrombosis
Approach
Microsurgical model and skills assessments
The participants will perform end-to-end anastomosis of chicken wing arteries using standardized microsurgical instruments and 9-0 monofilament sutures under microscopes. Each anastomosis will be assessed by two experts blinded to the participant’s identity.

From Hino A. Neurosurgery 2003;52(6):1495-1497.
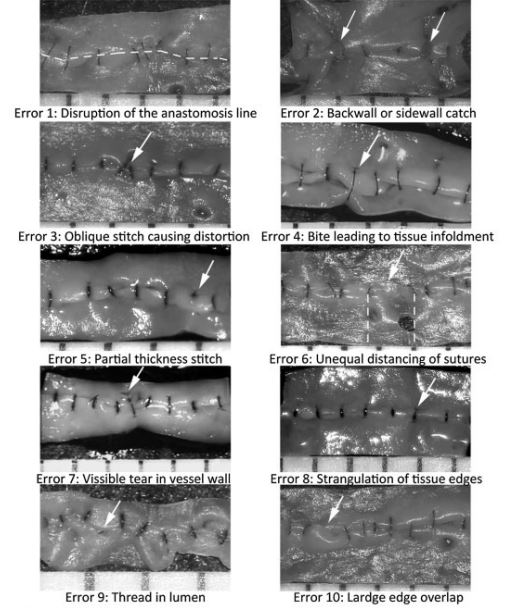
Upon completion, each anastomosis will be cut longitudinally to view the intimal side and we will use the subjective ALI score to evaluate visuo-spatial ability. By opening the vessel at the end of the procedure and examining the regularity and structural architecture of the end product, Ghanem et al. were able to assess microsurgical skill through the identification of 10 errors that would lead to anastomotic failure such as leaking or thrombosis. Based on these 10 errors, an Anastomosis Lapse Index (ALI) was created and a pictorial representation of each error and a simple index to refer to the level of competency achieved was presented.

Manual evaluation of microsurgical anastomosis is both time-consuming and prone to bias. To address this, in this paper we propose an automated and quantitative framework that uses image processing and geometric modeling to detect ALI errors. Leveraging high-quality datasets from two collaborating medical institutions, our method replaces subjective expert scoring with an objective pipeline that reliably identifies and quantifies five key surgical errors. Results demonstrate that the system closely matches expert evaluations while providing consistent, stitch-level feedback to support microsurgical training

From Ghanem AM, et al. J Reconstr Microsurg. 2016;32(3):233-41.
Recording of motion, force and EMG activity
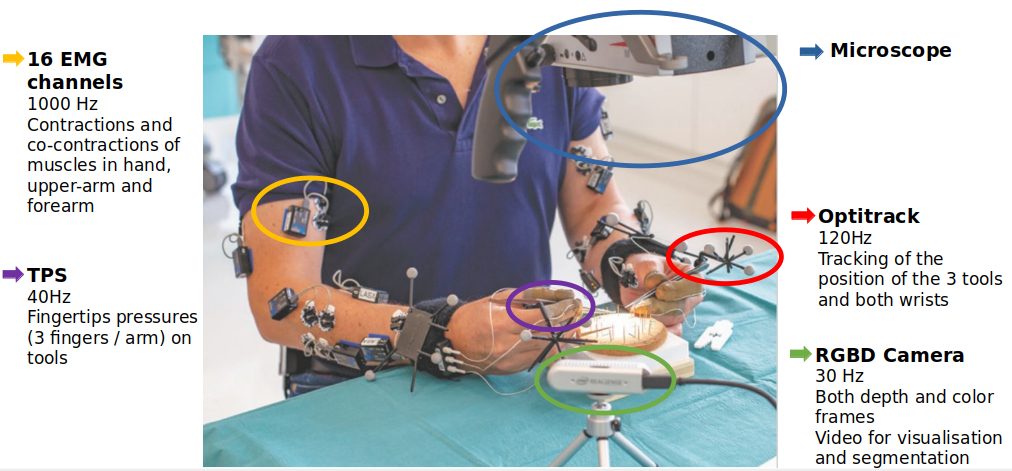
The participants will use microsurgical instruments with motion sensors and wear force sensors and muscle activity sensors. To study motion, we will use a high-resolution set of cameras tracking small markers mounted on the surgeons’ wrists and surgical tools.
We here opt to use Optitrack which offers high resolution tracking (360 frames per seconds and millimetric accuracy). We will use indirect information on the force produced by the surgeons like measurements of muscle contraction (by EMG) and the pressure applied on the tools. We hence seek to derive variations of forces generated during the surgical procedure.
The recording setup includes: an external RGBD camera which provided depth and color frames at 30Hz, used to segment manually the operation phases, an Optitrack set of cameras with markers, used to track precisely motion of hands and tools, EMG sensors on both arms (8 channels recorded at 1000Hz) and TPS fingertip pressure sensors, placed alongside the thumb, index and middle fingers.
In our research, we developed a framework that enables accurate skill assessment and provides objective feedback for improving microsurgical anastomosis skills among surgical trainees.
We show that the proposed set of objective and quantitative metrics to assess skill proficiency aligns with subjective evaluations, particularly the ALI score method, and can effectively differentiate novices from more proficient microsurgeons. Furthermore, we find statistically significant disparities, where microsurgeons with intermediate level of skill proficiency surpassed novices in both task speed, reduced idle time, and smoother, briefer hand displacements.


Interplay between human motor skills and microsurgical performance
In our earlier investigations, we introduced an image-based framework that automatically detects microsurgical errors and evaluates surgeon proficiency using quantitative metrics such as motion smoothness. This raises the challenging scientific question of why expert surgeons can perform with smoother motion, higher efficiency, and a lower incidence of ALI errors.
To address this question, it is essential to acknowledge that microvascular anastomosis is an inherently complex procedure, demanding precise planning and continuous coordination among the surgeon’s hands, instruments, the needle, and the vessel. The procedure can be decomposed into distinct sub-steps, each defined by the information available to the surgeon, the motion dynamics, and the evolving needle–vessel interaction.
By adopting this fine-grained perspective, it becomes possible to elucidate the mechanisms through which specific motor skill deficiencies give rise to characteristic microsurgical errors, thereby linking observable performance metrics to the underlying principles of human motor skills.



Beyond fine-grained manipulation skills, surgeons rely heavily on a visual feedback loop to determine insertion targets, servo the needle tip toward the desired location, and continuously estimate the configuration of the needle and vessel in real time. The effectiveness of this loop is strongly influenced by visuospatial ability. Such skills are broadly present and frequently refined in daily life; however, in microsurgery, they take on a unique dimension, as all operations are conducted under magnification. This setting introduces a novel mapping relationship between perception and action that must be gradually acquired through practice.
To study the acquisition of this skill, we devised a controlled 2D path-tracking task in which participants were asked to precisely follow a star-shaped pattern under different magnification ratios. Prior work in laparoscopic surgery has shown that familiarity with a reference frame facilitates surgeons’ adaptation to new visual–motor mappings. Building on this, our aim is to understand how surgeons balance the trade-off between achieving high accuracy under high magnification versus maintaining a wider field of view under low magnification, which provides richer contextual information for mental visualization of the reference frame.
To support this investigation, we have also developed a computer vision–based framework capable of tracking the surgical tool tip in real time, enabling precise quantification of visuomotor performance under varying visual conditions.

Publications
You will find the list of related publications here.