The operating theatre of a hospital is an area that most people will try to avoid as much as possible during their whole life, as in most cases when one is needed, it does not emit a positive signal concerning a person’s health. For a smaller group of people, doctors and nurses mostly, an operating theatre is part of their everyday work environment as they tend to the needs of the first group of people mentioned.
For both patients and staff, it is absolutely vital that the environment of an operating theatre responds to the highest hygienic and safety standards, especially concerning the indoor air quality, as the patients can be in a physically weak or fragile state, and the medical personnel can find themselves handling hazardous products while in the operating room and during surgery.
But these two groups are not at risk from the same substances and should not care about the same parameters when it comes to the indoor air quality of operating theatres. Patients are mostly already in a weak physical state where their immune system is likely to be working only at a reduced level. Therefore, patients are at a higher risk of catching an infection or an illness from airborne biological agents. According to a study by S. Cabo Verde et al. (2015) [1] on the microbiological air quality of various hospital sites, gram-positive cocci were present in 78 % of the samples taken from operating theatres, staphylococcus in 55 % of those samples, and gram-negative cocci in 23 % of the measurements. The presence of bacteria in operating theatres does not always have to lead to infections in patients, but it seems logic that the less bacteria are present, the less likely is a nosocomial infection.
In order to reduce the number of bacteria in the air, it is important that the room is clean and does not present any bacterial sources within, which could be suspended by the air movement due to the ventilation. To further reduce the risk of accidental infection, Leung and Chan (2006) [2] suggest that the air supply into the operating theatre be in the form of a laminar flow in a vertical, downwards direction, as is shown in figure 1. This unidirectional airflow ensures that the patient receives clean air which has come directly from the ventilation system, and that has not had the possibility to flow past sources of contamination and suspend them.
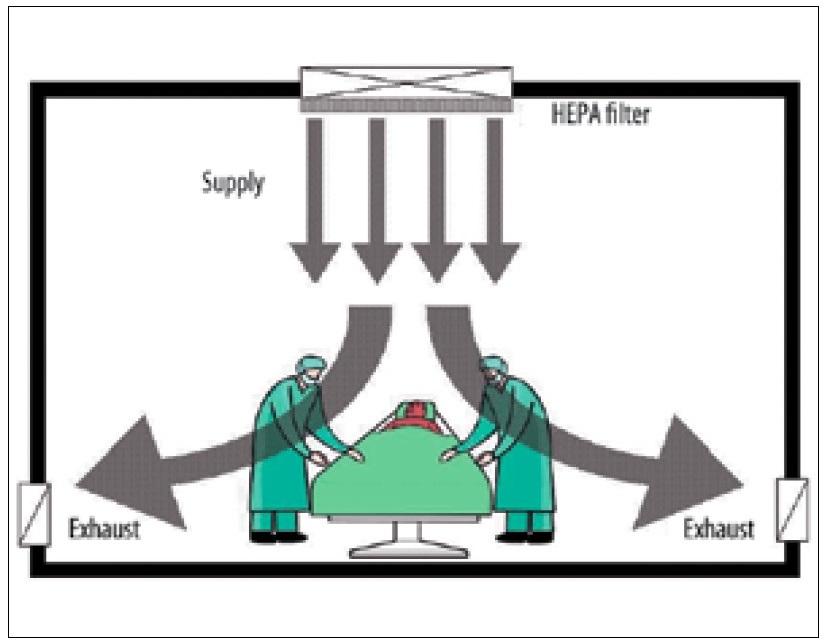
Figure 1: Ventilation air supply in operating theatre. Source: Leung and Chan (2006)
But in order for the airflow management to make any sense, the air which is supplied to the room should be as pure as possible and present the least possible traces of bacteria. This means that the air supply system must be clean and functional and not itself have sources of contamination within, such as dirty air ducts. Good planning and regular maintenance of the system are the best methods to ensure that this does not become the case. Leung and Chan (2006) also suggest using a series of filters and an ultraviolet germicidal irradiation system (UVGI) in the air management unit. There should be a combination of a normal filter and a high efficiency (HEPA) filter, to reach the best performance possible. The UVGI system is used to damage the DNA of bacteria suspended in the airflow, thus rendering them harmless if they are to come into contact with the patient. So that there is no “old” air, which is more likely to by polluted in the operating room, the air management system should have an air flow rate of at least 15 air changes per hour of outdoor air [3]. A schematic of such a system is shown in figure 2.
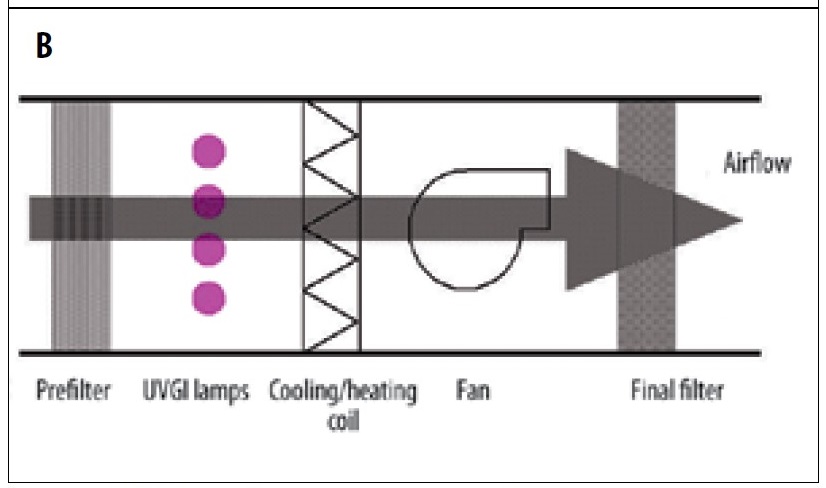
Figure 2: Air treatment within the air management system. Source: Leung and Chan (2006)
The personnel present in the operating theatre are naturally also subjected to the various bacterial sources, but this is not critical for them, as their immune systems are robust enough to deal with the threats. A more concerning source of air pollution for doctors and nurses while operating a patient is anaesthetic gases which escape from the applicator used by the patient. Obviously, accidental exposure to anaesthetic gases is of no concern to the patient, as the aim is for them to inhale the gases. Common anaesthetic gases are halothane (CF3CClBrH), isoflurane (CF3CHClOF2H) and nitrous oxide (N2O), among others. There is still controversy on whether the exposure to traces of anaesthetic gases is dangerous to the health of doctors and other operating room personnel, but some studies have implicated the exposure to these gases in having adverse health effects, such as liver and kidney damage, spontaneous abortions and birth defects, short-term memory impairment, and an increased risk of genetic damages [4].
The most efficient solution to reduce the amount of anaesthetic gases in the air of operating rooms is to use an anaesthetic gas scavenging system (AGSS). They are complete systems that are used to capture excess or leaked gases from the patient’s respiratory tract used to administer the anaesthetic, and then expulse them through a non-recirculating air vent. These systems are common in modern hospitals and generally function very well. There are concerns, though, about older health care facilities, where the efficiency of an AGSS installed a long time after construction of the hospital may be insufficient to meet all standards [4]. Poor work practices and inadequate or insufficient maintenance of the AGSS leads to higher concentrations of gases in operating theatres.
The two sources of air pollution mentioned in this post are in most cases the predominant sources of bad indoor air quality in most operating theatres. But it is important not to only focus on theses sources, because others exist, and which in certain cases can lead to dangerous exposure levels for both the patient and the medical staff. One of these other sources are cleaning and disinfectant products used to clean operating theatres. Two chemicals often measured in disinfectant products are formaldehyde and glutaraldehyde, both known to have adverse health effects.
To reduce the exposure in operating rooms to any of the aforementioned hazardous substances, it is important to respect the various recommendations about the ventilation systems, and to perform regular and effective maintenance of the air management systems, to avoid them becoming under-performant. We have the technology necessary to achieve a very safe air quality in operating rooms, but for it to be effective, it must be installed, maintained, and used according to the latest knowledge available in the domain.
References
| [1] |
S. Cabo Verde, S. M. Almeida, J. Matos, D. Guerreiro, M. Meneses, T. Faria, D. Botelh, M. Santos et C. Viegas, «Microbiological assessment of indoor air quality at different hospital sites,» Research in Microbiology, vol. 166, pp. 557-563, 2015. |
| [2] |
M. Leung and A. H. Chan, «Control and management of hospital indoor air quality,» Med Sci Monit, vol. 12, n° 13, pp. 17-23, 2006. |
| [3] |
ASHRAE, «Chapter 7 – Health Care Facilities,» chez ASHRAE Handbook: HVAC Application, Fundamentals, Atlanta, American Society of Heating, Refrigerating and Air-Conditioning Engineers, 1999. |
| [4] |
E. G. Dascalaki, A. Lagoudi, C. A. Balaras et A. G. Gaglia, «Air quality in hospital operating rooms,» Building and Environment, vol. 43, pp. 1945-1952, 2008. |